The Why and How of Thyroid Dosing
Thyroid assessment and treatment
Your thyroid is a master controller of vital human functions. It controls your rate of metabolism and is the seat of your immunity. There is an array of firmly held opinions, explanations and approach to treatment.
Characterization and symptoms
Hypothyroidism, an under active thyroid gland, is common and is a frequently under-treated or un-treated endocrine disorder. It is characterized by any of a number of symptoms including:
- fatigue
- weight gain or inability to lose weight
- depression
- poor immunity
- cold hands or feet
- hair loss
- dry skin
- low body temperatures
- constipation
- cognitive impairment (foggy brain)
- puffy eyelids or loss of lateral eyebrows
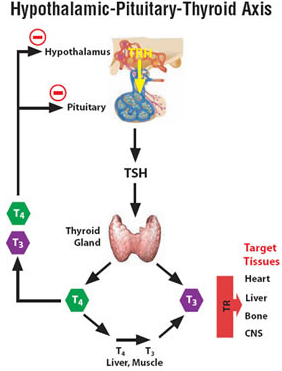
Thyroid Cascade and Control
The approach to thyroid disorders is steeped in tradition, dogma and lack of understating of basic physiology and biochemistry.
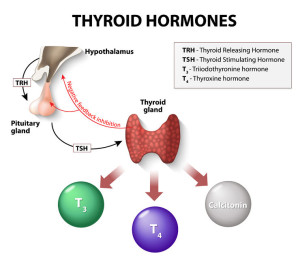
The thyroid is part of a sequence of controllers as shown in the diagram above . Thyrotrophic releasing hormone TRH is hypothalamic based. It regulates the pituitary to secrete TSH (thyrotrophic stimulating hormone). TSH stimulates the thyroid to secrete T4. T4 is converted to T3 (the active hormone) partly in the thyroid but primarily in the liver then muscles and other organs by a series of D1, D2 and D3 (deiodonase enzymes). This is an idealized feedback loop.
It does not always works this elegantly. At every step there can be a dysfunction.
Testing
In today’s cost-conscious penny-pinching environment controlled by your insurance company (to whom you have given total control), the TSH alone has become the preferred method of screening thyroid status — because it is a cheap test. It is an inadequate and poor screening measure.
You are being short changed. You cannot rely solely on the TSH to accurately assess true thyroid function.
The pituitary TSH and thyroid T4 / T3 move in opposite directions. That is the feedback loop. High TSH is produced by low thyroid (hypothyroid). A low TSH would result from an over-active thyroid (hyperthyroid). Again, it is not always this simple. That is the basic flaw in medical thinking.
To adequately assess true thyroid status you need run or request the following tests:
- TSH
- free T4 (not total T4)
- free T3 (not total T3)
- thyroid antibodies
- reverse T3
Again, free T3 is the active fraction. That is what is being overlooked. More attention has been focused on this problem. I see more psychiatrists recognizing this schema and treating depressive disorders with T3.
Unfortunately, the common thinking (not wisdom) is T4 will always convert to T3, so don’t worry about it. False premise
Therapy and Pharmacological Approach
What are pure T4 drugs? These are staple of conventional medicine.
- levo-thyroxine (generic)
- Synthroid
- Levoxyl
- Tirosint
Every pharmacist will tell you they are identical. This is not true. Thyroid preps are notoriously difficult to standardize. The major manufacturers have had to recall huge lots of Synthroid and Levoxyl over the years because of standardization problems. And patients can easily tell the difference in efficacy and potency between every one of these drugs. Absorption differences because of tableting, binding constants, excipients and fillers. You are most often being prescribed the cheapest of them all — levo-thyroxine which is the least standardized. Tirosint is the purest form.
What are pure T3 drugs?
- Cytomel (liothyronine) — very short acting
- Compounded long acting T3 (tri-iodothyronine) — sustained action
And combinations. These are the staple of most “alternative” practitioners.
- Armour thyroid (desiccated thyroid)
- Naturethroid
- Westhroid
- Thyrolar
- Compounded T4/T3 combination
Integrative and Rational Approach
Now what do we do with all this information and set of approaches? There is a common “wisdom” in the conventional endocrinology or internal medicine community that any use of desiccated Armour Thyroid is quackery. Why would anyone use such an outdated approach? And this has been forcefully articulated in the past by noted University Stanford Professors. In the alternative community the obverse dogma holds. Anyone who does not use desiccated thyroid or combinations is not very creative or knowledgeable. What is the correct approach?
It is a rational and empirical approach. Do what the patient and the situation dictate. The old aphorism articulated by the late great Sir William Osler:
Listen to your patient, he is telling you the diagnosis. — Sir William Osler 1849-1919
It is a combination of listening to the set of symptoms and matching to the appropriate lab profile. At its best an empirical art form with rational starting points.
Proprietary Conversion Ratio T3/T4
To guide our initial dosing we use a proprietary ratio. What is the ratio of (free T3 in pg/ml)/(free T4 in pg/ml). The pg/ml is important because the free T4 is always reported inappropriately in ng/ml while the free T3 is often reported in pg/ml. Different scalar units. Multiple the Free T4 (ng/ml) x 10 = pg/ml so we can compare in similar units. A healthy ratio is >25%. A low and inadequate ratio is <20%. That infers poor conversion of T4 to T3 and the need for additional T3. If the ratio is >= 25% then a pure T4 is sufficient.
Example:
Free T4 = 0.91 ng/ml
Free T3 = 2.7 pg/ml
0.91 ng/ml x 10 = 9.1 pg/ml
So 2.7/9.1 = 29.6% (very healthy)
In the end we frequently enter a trial and error period. Gradually advancing doses and then combinations as tolerated by you the patient. How are you responding?
Let’s continue this in the next post soon. We will elaborate on Hashimoto’s auto immune thyroiditis and Reverse T3 dysfunctions.
Philip Lee Miller, MD
Monterey CA
April 10, 2016
4 thoughts on “The Why and How of Thyroid Dosing”
Would the example above not be typical results in someone on T3+T4? This is exactly what mine look like on NDT, but never on T4 only drugs.
Thank you for writing. And apologies for missing this comment a few months ago. The most significant and easiest treatment of Hashimoto’s is gluten restriction. Then aggressively treating thyroid by “putting the thyroid to rest.” You can write to me personally at [email protected]
Thank you for writing. The blog is quite rich with details. It is rational approach to thyroid therapy and testing. The key to Hashimoto’s is gluten restriction.
I would like to hear more i have hasimotos.