Hashimoto’s Thyroiditis and Reverse T3 Thyroid
Hashimoto’s Auto Immune Thyroiditis
Hashimoto’s is an auto-immune condition. Where your body sees thyroid as “foreign” or “not self.” This stimulates production of antibodies against to your own thyroid. There are a host of auto immune conditions including Sjogren’s (Sicca Syndrome). Lupus, Scleroderma, CREST Syndrome and Rheumatoid Arthritis.
[Important note: It is vital to recognize that the TSH test is being used as a screening test. See previous blog. It will not diagnose Hashimoto’s. It will totally miss this condition for years.]
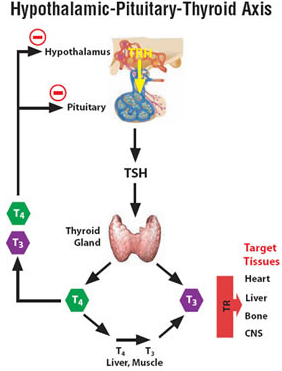
We measure two antibodies. Anti-thyroglobulin (matrix of the thyroid gland) and TPO (thyroid peroxidase). TPO is essential to the conversion of T4 to T3. Either of these can rise with Hashimoto’s. It is more common to see a rise in the TPO. This condition usually results in Hypothyroidism (under active thyroid) by interfering with the normal conversions. The normal flow is T4 converts to the active form T3. The more technical term is Hashimoto’s Autoimmune Thyroiditis. It can occasionally result in the opposite. That is, hyperthyroidism (over active thyroid) during a more acute or sub acute inflammatory phase. Thyroiditis means inflammation of the thyroid.
What causes Hashimoto’s? This is not really well known. There are various theories. You will read that there are genetic factors. And, it is far more common in women than men. It is quite unusual in men.
Speculative (unproven) theories
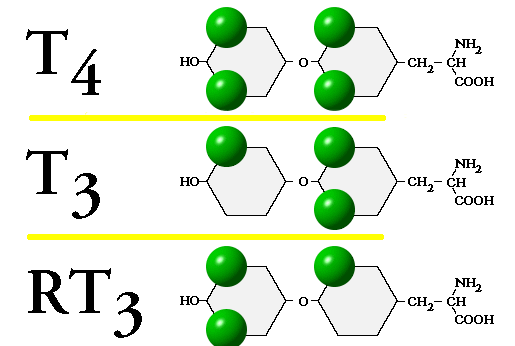
- Halides (group VIIa of the periodic chart) — bromine, fluorine, and Iodine. Iodine is the key constituent of thyroid. T4 (tetra-iodo-thyronine) has 4 iodine molecules. T3 (tri-iodo-thyronine) has 3 iodines. Bromide, Fluoride and Choline (all halides) might interfere with the actions of iodine. Bromide is found in bread, Fluoride is found in drinking water and toothpaste. Chorine and chloride are ubiquitous.
- Gluten sensitivity. This is empirically quite real. Every patient treated with a gluten free diet will experience a fall in antibodies levels. We theorize that gluten adheres to the gut enteric wall. This induces an auto immune response. The thyroid is a key target of all auto immune responses.
- Post-partum transfer of fetal blood during delivery. This was a common theory. Tiny amounts of blood from fetal circulation induce an auto-immune response. This does not explain why men develop Hashimoto’s
- Could estrogen play a role? It is far more common in women than men.
Treatment of Hashimoto’s Thyroiditis
The goal is “put the thyroid at rest.” A gluten free diet is essential And then aggressive thyroid suppression. Let’s define basic therapeutic forms:
Pure T4 (none of these are identical):
- levo-Thyroxine (generic)
- Synthroid
- Levoxyl
- Tirosint
Pure T3
- Liothyronine (Cytomel) — a synthetic
- Tri-iodo-l-thyronine
Mixed T3 and T4 (usually desiccated):
- Desiccated Thyroid (Avicel)
- Armour Thyroid
- NatureThroid
- Westhroid
- Thyrolar
Antibody formation can be reduced by suppressing the TSH. This is done by increasing T4 and T3. That down-regulates the auto immune response. We can treat with a pure T4. Occasionally, treat with a combination T3/T4. Or a pure T3 (compounded tri-iodo-l-thyronine) . See previous blog discussion. This is based on absolute T3 values and the ratio of T3/T4. We reject by rigid orthodoxy or dogmatic thinking. Treating you, the patient, based on your own situation.
A New Novel Treatment – LDN
More recently, another more novel approach has proven successful. Low dose Naltrexone (LDN). At high doses, Naltrexone is an opioid and endorphin inhibitor. It reverses opioid over-doses. But at very low doses it has the opposite effect. It has a transient blocking effect. That causes a physiologic counter-reaction. So it increases endorphins (the feel good hormone neuro-transmitter). There seems to be a connection with increased endorphins and mitigation of auto-immune conditions. Hashimoto’s and Crohn’s are the most significant targets. Now here is some additional reading — The LDN Book.
How Does Reverse T3 Cause Hypothyroidism?
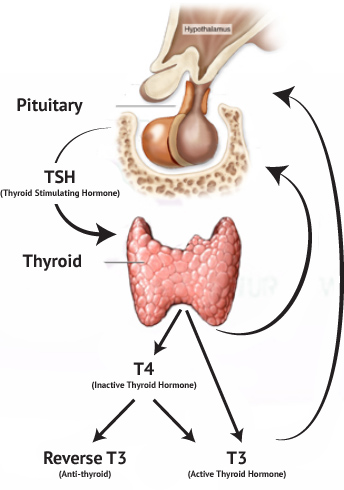
Reverse T3 is over expressed by stress or internal imbalances (selenium deficiency). The RT3 is a mirror image of T3. It can interfere (compete) with the physiologic action of T3. This can cause hypothyroidism even if the T3 appears to be normal.
Through empirical observation, we have found that treating abnormal RT3 with a pure T4 will only worsen the condition. It will increase the production of more RT3. So a pure T3 is a better and more rational approach. It by-passes this pathological conversion state.
This is another instance where a simple TSH screening is inadequate. It will fail to diagnose this condition. Therefore, we repeat again. Ask for a complete and comprehensive thyroid lab survey. What does that include? You want a free T4, free T3, thyroid antibodies and reverse T3. This concludes part 3 of our thyroid series.
16 thoughts on “Hashimoto’s Thyroiditis and Reverse T3 Thyroid”
Thank you for your comments. Your TSH is fully suppressed. Based on this value some endocrinologists would lower your thyroid dosing. However, your free T4 and free T3 are fairly healthy. Certainly not toxic. So I would not be concerned about your suppressed TSH. Your thyroid and TPO antibodies indicate you do not have Hashimoto’s.
The reverse T3 is only mildly elevated depending on your lab range. There is controversy regarding reverse T3. Reverse T3 will compete with T3. So the bottom line is — how do you feel? You may need some additional T3. This will improve the cold hands, cold feet, digestive problems, cognitive problems, energy levels and sense of well-being.
Philip Lee Miller, MD
The doctors have said my labs make no sense and cannot figure out a plan ahead. My thyroid was removed at age 19. I am not 62. I am currently on both T3 and T4. I am a bit baffled by the high RT3 and do not understand if the RT3 is actually competing with the T3 sites and impacting TSH or if it just an inactive form in my cells and not to worry. Thanks!
TSH = <.006
T3 Free = 2.8
T4 Free = 1.24
Thyroglobulin Antibody = <1.0
RT3 = 27.1
TPO Ab = 10
Body Temp 96.2 F in morning up to 97.6 daily
Thank you for writing. These are always complex situations. Your thyroid numbers alone are “within range.” There is no evidence of Hashimoto’s. Your estradiol is very low which could account for hair loss. This is probably more menopausal than hypothyroid. That is what you need to pursue.
I am in Australia. These are my results. Can you let me know if these fall within normal range? I am constantly fatigued, thinning hair and eyebrows, intolerance to heat, significant weight gain. I am 57 years old
FT4 14.5 pmol/L
TSH 1.53 mIU/L
FT3 4.7 pmol/L
TG Antibodies <15 U/ml
TPO Antibodies 34 U/ml
Reverse T3 304 pmol/L
Oestridol < 60 pmol/L
Cortisol 485 nmol/L
The closest thing I have ever equated with my issues are a “mild” form of hashimotos. No positive blood tests, just symptoms alone.
My rt3 is always slightly high, TSH low, and T4 normal or high.
T3 makes me feel way worse. Iodine at first helped (at high doses), then a few days later I crashed and went hypo.
Levoxyl brand t4 seems to slightly help me, and I have no idea why, as I’m still producing high rt3. The reason is probably because it’s much more complicated than that. I feel much worse with lower RT3 and higher FT3.
I just started being treated for Hashimoto’s because of these results. It is all very confusing to me. In your opinion, do these results say Hashimoto’s?
T4 free 1.26
TSH 5.3
reverse T3 21.5
vitamin D 5.8
TPO 133
T3 free 2.3
Thank you for your time and dedication.
Thank you for writing and apologies for any delay. This is a complex set of numbers but an excellent example why the TSH alone is an inadequate measure of thyroid function. Your TSH is “normal.” But your thyroid is definitely not “normal.” Have you been told all these numbers indicate a normal Thyroid? It appears that you have Hashimoto’s autoimmune thyroiditis. With a T3 indicating it might be slightly over active rather than underactive. Your vitamin D is bit over the “sufficient” range in Feb. Your RT3 (reverse T3) is not abnormal.
Contact me personally at [email protected]
Hi there,
I’ve had thyroid symptoms for years and always had normal TSH tests so was told it was “anxiety”. I’ve recently insisted on more thorough lab work with these results:
Feb 2018 TSH 1.92 Nov 2018 TSH 1.18
Feb 2018 TPO 78 Nov 2018 TPO 134
Feb 2018 ThAb 12 Nov 2018 ThAb 13
Feb 2018 Th 51 Nov 2018 Th 36
Feb 2018 ferritin 105 Nov 2018 ferritin 71
Feb 2018 vit D 107 Nov 2018 vit D 84
Nov 2018 FreeT3 3.82
Nov 2018 FreeT4 12.5
Nov 2018 RT3 26
Does this indicate a problem with my thryoid?
Thanks
Thank you for posting. I cannot give you a complete answer. There is no free T4. And you did not include thyroid antibodies. At first glance, these numbers appear to be “normal.” And I do not know whether you are being treated with any thyroid preparation. There are instances where thyroid numbers are completely “normal” but the patient still suffers from clinical hypothyroidism. In the literature this is called subclinical hypothyroidism. But rather refers to the inability to completely diagnose thyroid dysfunction strictly with numbers alone.
This is where the therapy of thyroid dysfunction requires experience and an integrative approach. You can write me directly at [email protected] for more discussion.
Thank you for writing. There has been some significant discussion of interference with thyroid testing and the B vitamin biotin. Biotin is very important when taking large doses of alpha lipoic acid. But apparently it can interfere with thyroid testing. It is a complex process. Personally, I have not been able to identify this problem. But it is being reported with increasing frequency.
Here’s an interesting quote:
So in all likelihood, that is what they are referencing. Ask for a repeat or a more detailed explanation. And then write back to me again.
I recently got my thyroid tests back and the lab could not test my reverse T3 because something in my blood work was interfering with the test.
What would cause this and what should I be asking my doctor to do now?
Can you explain my results
Free T3/ Reverse T3 Ratio 2.68
Free T3 330 pg/dL
Reverse T3 123 pg/mL
TSH (Refl) 1.09 mIU/L
I am constantly gaining weight, losing tons of hair, and loss of appetite.
Thank you for writing. It is difficult to give you a precise answer. It is obvious that you have hypothyroidism. I cannot tell the degree to which you are suffering from Hashimoto’s as the antibodies are not stated here. You have used various combinations. We use long acting triiodothyronine which may be the same as sustained action liothyronine. Simple liothyronine (Cytomel) is too short acting and ineffective as it must be dosed three times daily. We also find Levoxyl or Tirosint is superior to Synthroid.
There may be other factors in your pain syndrome. This is a challenging problem. You may want to call us for further information and relief.
Hello,
I have Hashemite disease. My last blood test was 5 weeks ago
TSH was 19
T3 b
About 2
I’ve been on Armor prior to last blood test and it absolutely worsened my levels
I’m now on 175 mcg synthroid &
(2) 5 mcg in the AM Liothyronine
I am experiencing a level 15 with my periphal & brachial neuropathy
I am usually at a 8 pain level and take (4) methadone a day
I’m severely fatigued and has worsened since the Liothyronine
Thank you for your comments. Everyone is an individual. I demonstrate that my approach is flexible for each patient. There is no one size fits all. There is a rational approach to determining which preparation is appropriate for you.
I have been successfully treated for hypothyroidism with WP Thyroid , which is produced by the same company that makes Naturethryoid.
TSH is irrelevant. the free T4 should be in a low normal range; Free T3 should be in the high normal range;reverse T3 should not be elevated. and obviously your hair should not be falling out-you should not be having any body temperature dysregulations, with ice cold freezing and shivering and body temps really low such as 96’s or below 97.8 and with temps reaching at least 98.6 during waking hours with higher at some activities. I had the antibody and tpo tests Free and total T4 and T3, reverse T3, T3 uptake, and a lipid panel.When taking WP thyroid my lipids became optimal. WP thyroid has no artificial ingredients as armour thyroid does. The only additives in WP thyroid are mct oil and some fiber from chikory.